
As the United States approaches the occasion of its ‘One Millionth Covid Death’, the US corporate press is certain to bombard the American public with commemorations and loud reminders of this morbid milestone.
Just as major media continuously pounded the official narrative of the Covid terror into the public psyche for months, through running tallies on the scoreboard of death presented on each evening’s news broadcast, the coming media blitz will strive to burn the Covid scars into the public mind forever.
As the seminal event in US public health history, the crisis and its horrors, real or imagined, must remain in our psyche forever, as well as the heroic efforts we are told softened this epidemiological nightmare.
But mostly the behavioral management teams that create these narratives need us to remain vigilant and fearful for the next crisis, which is always lurking right around the corner.
Throughout this non-stop barrage of media fear-mongering and psychological manipulation one important item has been missing- that most vital of questions- a question so glaringly obvious yet kept off the news reports and notably absent from all “acceptable” discussion:
“What exactly counts as a Covid-19 death?”
To fully understand what a Covid death is- and what it isn’t- it is essential to understand the radical, and to this day unexplained, changes made in how deaths would be recorded, starting in the Spring of 2020. For the last two decades, standardized cataloging of mortality statistics has been in place, as outlined in the CDC’s Medical Examiners’ & Coroners’ Handbook on Death Registration and Fetal Death Reporting and the CDC’s Physicians’ Handbook on Medical Certification of Death.
The arrival of Covid-19 would usher in a new manner of recording mortality.
On March 24th, 2020, the National Vital Statistics System (NVSS), under the direction of the CDC, issued ‘COVID-19 Alert No. 2’ to all physicians, medical examiners, and coroners as a guideline as to ‘how cause of death’ would now be reported on death certificates, exclusively for COVID-19.
The Alert states the following:
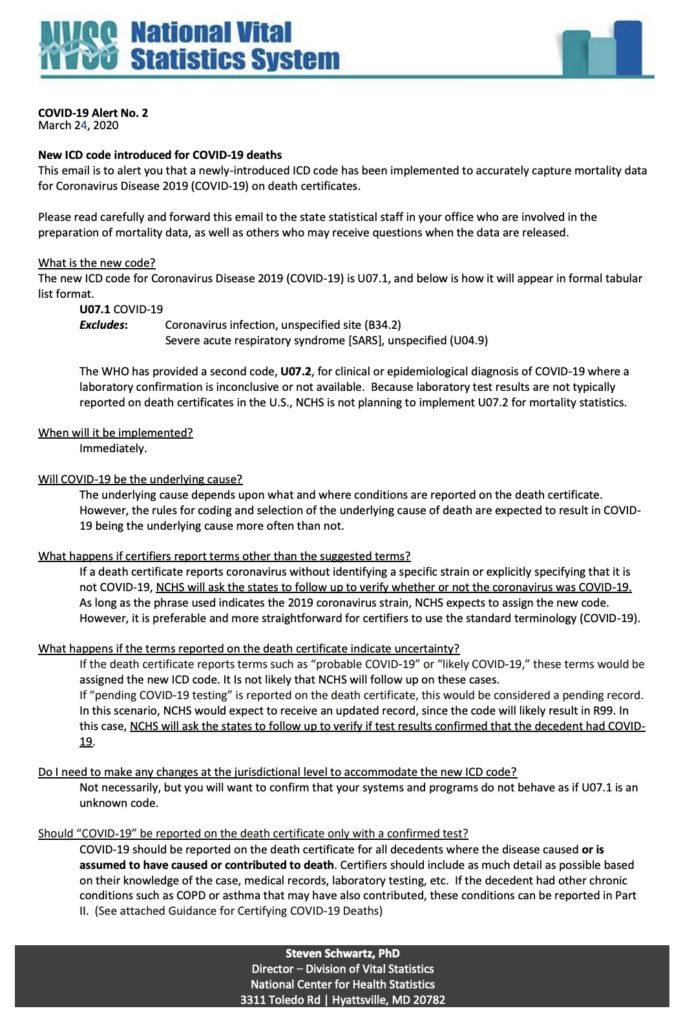
The ramifications of this can not be overstated as the NVSS, a division of the CDC sets the rules for how state health departments are obliged to assess mortality data.
This seemingly innocent single-page release became a watershed moment in how the United States would define Covid-19 deaths and began a process by which all manner of deaths would be coded as U07.1 COVID-19.
In practice, this led to a grossly exaggerated number of deaths being mislabelled “Covid-19 deaths.”
For example, as of Feb. 3rd, 2021, a glimpse at Table 3 of the CDC’s “Conditions Contributing to Deaths Involving COVID-19” shows 14,369 deaths listed as injury deaths which were recorded in the Covid-19 death count. While not the largest example of Covid-19 death misattribution, this clearly illustrates the deceit and manipulation which is found throughout the CDC Covid-19 mortality database.
Further examples of questionable accounting found in the CDC’s Provisional Mortality Statistics Covid-19 database can be found here– 1,265 deaths in 2020-2021 occurring from falls from various structures coded as U07.1 (COVID-19); and here– 17 drowning deaths all coded U07.1 (COVID-19); and here– 99 suicides all coded U07.1 (COVID-19).
Such examples are not unique. An exhaustive examination of the CDC’s Provisional Mortality Statistics database reveals that finding a case where an individual died solely from Covid is the exception. Based on all we now know, questioning any and all deaths attributed to “Covid” is imperative.
In a press conference back in April 2020, the director of the Illinois Department of Public Health, Dr. Ngozi Ezike publicly (and possibly inadvertently) admitted outright to the overcounting when she stated:
“If you were in hospice and had already been given a few weeks to live, and then you also were found to have COVID, that would be counted as a COVID death. It means technically even if you died of a clear alternate cause, but you had COVID at the same time, it’s still listed as a COVID death. So, everyone who’s listed as a COVID death doesn’t mean that that was the cause of the death, but they had COVID at the time of the death.”
Similar remarks were made by Maricopa County Public Health Executive Director, Marcy Flanagan highlighting the fungible manner in which health departments throughout the country recorded Covid deaths.
Shortly after the CDC issued its new guidelines the World Health Organization, on April 16th, 2020, would release its own document titled, “International Guidelines for Certification and Classification (Coding) of Covid-19 as Cause of Death.”
The WHO’s guidelines would define a Covid-19 death as, “a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease.”
This vague definition allowed for a broad interpretation of what could be considered a Covid-19 death and would lead to an over-reporting of deaths from Covid-19 and the underreporting of deaths from other causes.
The guidance goes on: “A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.”
This is very important when considered in the context of how COVID-19 symptoms have been defined- fever, chills, cough, shortness of breath, fatigue, muscle aches, headache, loss of taste or smell, sore throat, nasal congestion or rhinorrhea, vomiting, or diarrhea, and skin rashes.
Physicians are being told here that, when they have identified a Covid-19 death, using the loose “if it looks like Covid” definition, regardless of any pre-existing conditions the death must be registered and counted as a Covid-19 death. This goes against all past protocols for identifying the cause of death. By simply recognizing symptoms, which correspond to many different ailments, the death is now registered as Covid-19. This is basically an ad hoc methodology never implemented before.
In addition to these alterations for the coding of Covid-19 deaths, physicians and hospitals were given financial incentives for labeling patients with COVID-19, and providers were given an array of codes for billing COVID-19 deaths.
Due to the new codification methodology implemented in countries across the world, it became expected and implicitly suggested that all types of deaths would be listed as Covid-19 deaths.
As far back as March 2020, Prof Walter Ricciardi, scientific adviser to Italy’s minister of health states:
“The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus. On re-evaluation by the National Institute of Health, only 12 percent of death certificates have shown a direct causality from coronavirus, while 88 percent of patients who have died have at least one pre-morbidity – many had two or three.”
Based on all we now know it is fair to question any and all deaths attributed to “Covid.” This illustrates that the covid death toll is rigged to show a higher fatality rate.
This brings us back to the fundamental question of how a Covid-19 death is defined. The answer to this question is of vital importance as it sheds light on the massive fraud that has accompanied the constant drumbeat of “The “Covid Death Toll.”
These fabricated numbers of deaths attributed to COVID-19 cannot be explained away as merely an accounting glitch. The Covid death numbers have been used by governments around the world to stoke public fear, create mass hysteria, justify draconian “lockdown” measures, impose mandates for experimental injections and impose continuous “states of emergency” which have launched an assault on our basic rights including bodily autonomy.
As we’ve established the grim reality that most COVID-19 deaths are actually NOT from COVID-19, there can be little doubt that the changes in the protocol were designed to increase the death rate in order to heighten public fear and anxiety.
And where does this leave us? Are we left to wonder how many of these deaths were actually from the virus called SARS-CoV-2?
How many of these “Covid deaths” are excess deaths, deaths over and above what would be expected without COVID-19?
How many of those deaths were the direct result of government action, actions such as transferring patients recovering from COVID-19 into nursing homes? How many avoidable deaths occurred because people were unable or unwilling to seek medical attention for strokes, heart disease, and other life-threatening afflictions?
The task of reparation and remembrance of the Covid Crisis must begin with an honest account of what constitutes a “Covid Death” and must include a recovery of the truth about those deaths from the lies in which they have been shrouded and buried.
Given what can only be seen as a deliberate attempt to inflate the Covid-19 death numbers, that task begins with a thorough audit of the CDC and a full investigation of the WHO.












