On Tuesday, June 25, 2024, Idaho’s Southwest District Health Board (SWDH) held its monthly meeting to discuss multiple agenda items, focusing primarily on guidelines for their proposed “Measles Response Plan.”
The board’s entire presentation can be viewed here. The conversation specific to the Measles Response Plan picks up at the 22-minute mark. The significance of this SWDH meeting, however, extends beyond simply the contents of the Response Plan. What is of special interest are the reservations about certain proposals that board members brought up. Of equal importance were their requests for more information before they agree to an action plan.
What opened as a seemingly standard collaboration of health bureaucrats evolved into a serious inquiry, where board members posed provocative questions about the necessity for such a program and expressed skepticism about the use of resources to execute the program.
Some board members were quick to place the “Measles Response Plan” in the context of the past four years. They emphasized the current climate of distrust in health authorities that the public harbors, given the injuries they witnessed or experienced from the recent covid vaccine program.
The hesitancy of these local officials to impulsively embrace a plan handed down to them can be seen as a message to national health bureaucrats. The message conveys to federal authorities that they may likely receive significant pushback from the general public if such a nationwide response plan were to materialize.
The interactions between the presenters and the health board seemed to represent a seismic shift from the way these discussions have been undertaken in the past. Such candid uncertainty toward the material presented offers an opportunity for health freedom advocates to educate both board members and the public on the historical evidence about measles, about the MMR vaccines, and about how health departments have been politicized and weaponized for the purpose of pushing broader agendas on Americans.
Measles National Update and SWDH Response Presentation
The Measles Response Plan opened with a slideshow presentation delivered by Public Health Program Manager (PHPM) Ricky Bowman and the guest speaker, epidemiologist Andy Nutting. They covered the major points of the “Measles National Update and SWDH Response.”
Bowman introduced the slideshow by announcing that there would be “an update with the national outbreak that’s going on, cost of measles and role of community partners.”
Nutting then began narrating the slideshow by going over the Idaho Department of Health and Welfare Rules (IDAPA 16.02.10). These rules set guidelines for reporting diseases to public health authorities and specify requirements for quarantine and isolation.
Nutting reported on the current state of measles in Idaho and nationwide. Inconsistent with Bowman’s assertion that there is currently a national outbreak of the measles, Nutting cited zero current measles cases in Idaho and a mere 151 alleged measles cases in the entire United States (population 330 million).
For some unknown reason, though, Nutting characterized the lone incident of a single household in Idaho in 2023 reportedly contracting the measles as an “outbreak.”
He then went on to show decidedly non-alarming current national statistics on the measles, which he again described as an “outbreak.”
While highlighting these nominal statistics, Nutting stressed that the highest percentage of those contracting the measles were unvaccinated children. But when reporting on hospitalization rates from the measles, Nutting admitted that the statistics were confusing.
While showing his final slide, which covered the “cost of measles,” Nutting admitted that “there’s very limited literature on the cost of measles” and that most of the literature “depicts the cost of measles for larger counties.” He also acknowledged that “perspectives weren’t necessarily aligned all across the board; some of the literature was specific only toward costs associated with direct cost of Health Care, others were specific to Public Health response and so on.”
He cited a figure of $32,805 as the “median cost per case” but provided no details as to how those costs were determined and no mention of how this cost might relate to or impact a smaller county.
Roles of Community Partners
Bowman followed up Nutting’s presentation by picking up on the theme of the costs involved in dealing with a measles case. He noted that, until the previous year, when that solitary household “outbreak” occurred, he had never seen a measles case in his public health career. The costs incurred, Bowman pointed out, were due to the time it took staff to identify contacts.
Expanding on this point, he highlighted what the roles of community partners would be if “there were a single case of measles in Southwest District’s Health Jurisdiction.”
Of particular concern to Bowman was the possibility that there could be “contact with the sheriff and prosecuting attorney in case we need to do any public health orders around isolation and quarantine.”
SWDH Preparedness and Response Efforts
Bowman wrapped up his portion of the slideshow presentation with a brief outline of “Preparedness and Response,” which highlighted how schools would handle an instance where a measles case and/or exposure was discovered.
On this point, it seemed Bowman was unclear. He perhaps misspoke when he stated, “Students that are not unvaccinated—I don’t have total guidelines—are required to isolate from the school for 21 days. There is a potential for post-exposure prophylaxis. If they have the vaccine within 72 hours[,] I believe that they can be back in school.”
The slide presentation, accompanied by Bowman’s commentary, indicated that, according to IDAPA guidelines, a “susceptible child will need to be excluded (from school) until vaccination is obtained.”
Neither Bowman nor Nutting talked about enforcement actions and what they might look like.
Health Board Discussion
At the conclusion of the presentation, the floor was opened for questions from board members.
Questions about the hospitalization rates and the infection fatality rates (IFR) of the measles were raised.
Board member Kelly Aberasturi recalled, “When we went through measles when I was a kid, I don’t think that maybe 10% of the people went to hospitals.”
While wondering why today’s hospitalization rates are so much higher, Aberasturi added, “In my family all my brothers and I got it. I have four brothers, and none of us went to the hospital. My neighbors have three children and none of them went to the hospital. So I just wonder.”
Board member Jim Tribble, MD, remarked to Aberasturi, “A lot of that I think what you might see is if you have a disease that is a hot topic like this with a lot of resources put into it, which is kind of scary, it pops up if somebody gets sick with that they’re often more likely to be directed and guided to the hospital.”
Dr. Tribble seemed to be suggesting that it is the amplification of fear, not the disease itself, that drives people to the hospital.
Dr. Tribble also asked, “What do we know the infection fatality rate is for measles, maybe on an age-stratified basis?” He added that, to his mind, the IFR should be the big guide in our response, because “What we’re doing here is putting a lot of resources into this for an outbreak of 150 people in a nation of 400 million people.”
He further clarified, “I mean, I wouldn’t call 150 nationwide an outbreak, but the potential is kind of what people are worried about.”
Because neither Bowman nor Nutting were able to answer Dr. Tribble’s questions, they agreed to come back with some hard data on the IFR rates.
As conversation turned to the response plan for Idaho public schools and the potential for a 21-day school quarantine, board member Viki Purdy warned: “This is the same nonsense we heard about covid, and it was a disaster. The response was a disaster. But this is exactly the same thing, and I would not like to see any of this stuff happen again.”
Other board members’ reservations were also readily apparent throughout the discussion. They had one particular exchange (scroll to the 58-to-59-minute mark) that highlighted how these dialogues have entered new territory.
Toward the end of the conversation, Dr. Tribble asked, “Do we have any long-term placebo-controlled randomly controlled trials with the MMR vaccine?”
To that question Nutting responded, “I don’t have any data like that off the top of my head right now.”
Dr. Tribble replied, “It’s also important to have a good understanding of the vaccine’s safety for the public, because a lot of people right now—we have to be realistic—are concerned about vaccine safety.”
Without missing a beat, Aberasturi chimed in, “There’s reasons for that.”
The answer to Dr. Tribble’s unanswered question, as noted in this fully referenced chart, is that there is not a single routine childhood vaccine that has been licensed based on long-term placebo-controlled trials, including the MMR vaccine.
As evidenced in the package insert and in Table 6 of the Supplementary Materials, M-M-R-II trials totaled only 834 children with a third developing gastrointestinal issues and a third experiencing respiratory issues. In the Priorix trial, both vaccine groups had high rates of serious adverse events, emergency room visits, and new chronic diseases (e.g., autoimmune disorders, asthma, type I diabetes, celiac, and allergies).
In an emphatic conclusion, Dr. Tribble said he “thinks that it is even more important to state and understand that they (federal health officials) misled health departments at a local level and that those are the enforcement arms of the policies. So, I think, as a health department in our area, it’s important that we ask critical questions, that we don’t take things on face value, that we know. The public needs to be educated, not told.”
What the education that Dr. Tribble is calling for looks like is more essential than ever. We’re at a turning point in the history of medical freedom. A wary public is waking up to the fact that many of the “accepted truths” handed to them by once-trusted medical practitioners and health officials are in fact paid promotions from an industry that puts its commercial interests above public health.
Misconceptions About the Measles
Despite the overall skepticism expressed and the relevant questions brought up by board members, their conversation was fraught with some fundamental assumptions about measles and the accompanying vaccination program that are unfortunately still presented as indisputable facts.
One such misconception repeatedly voiced in the meeting was the canard that measles cases in the US represent anything close to what could be called an “outbreak.”
The presenters never offered supporting data to back this claim of “outbreaks.” A modest amount of research shows that cases of the measles are rare in the US and have been for some time. A look at the CDC’s own data from 2000 to 2024, for instance, shows that measles cases rose above 200 in only three of those years—and this in a country of more than 300 million people.
Also overlooked in the SWDH meeting and in the larger national discussion about measles is the question of what actually defines a “measles case.”
Chapter 7 of the CDC’s Manual for the Surveillance of Vaccine-Preventable Diseases defines a measles case as “An acute illness characterized by: generalized, maculopapular rash lasting ≥3 days; and temperature ≥101°F or 38.3°C; and cough, coryza, or conjunctivitis.” In the fine print, the CDC states, “Temperature does not need to reach ≥101°F/38.3°C and rash does not need to last ≥3 days” in order to “confirm” a measles case. This definition calls into question the clinical specifics for what defines a “measles case.”
The Minnesota Department of Health has spoken to the problem of confirming a “measles case” based on clinical observation, noting, “Many U.S. health care providers have never seen a case of measles. Without proper laboratory testing, measles cannot be diagnosed.”
The Washington State Department of Health agrees: “Clinical diagnosis is unreliable, therefore cases must be laboratory confirmed.”
A 2006 paper from the UK also spoke to the need for laboratory testing. It said, “Clinical diagnosis of measles has a low positive predictive value [. . . and] laboratory testing is required to confirm the diagnosis.” The paper then added, “Other causes of fever and maculopapular rash include rubella, parvovirus B19, enterovirus, scarlet fever, human herpesvirus 6, human herpesvirus 7, Kawasaki’s disease, meningococcaemia, toxic shock syndrome, dengue, HIV, secondary syphilis, and drug eruptions.”
Even the tests are not considered failsafe evidence of a measles case, as detailed by the CDC: “There is no single serologic laboratory test capable of confirming with 100% confidence every true case of measles. Testing for measles-specific IgM from persons with rash and fever can produce false positive IgM results.”
The matter is complicated further when the CDC sends notifications to healthcare workers, many of whom have likely never seen a measles case, and tells them to be on the alert for “cases” of disease that meet the clinical criteria for a measles case—at the same time noting that the same criteria may fit other conditions.
Another commonly “known fact” that board members unquestioningly reiterated was the long-held fallacy that mass vaccination was responsible for eliminating mortality caused by the measles. The history and data tell a different story.
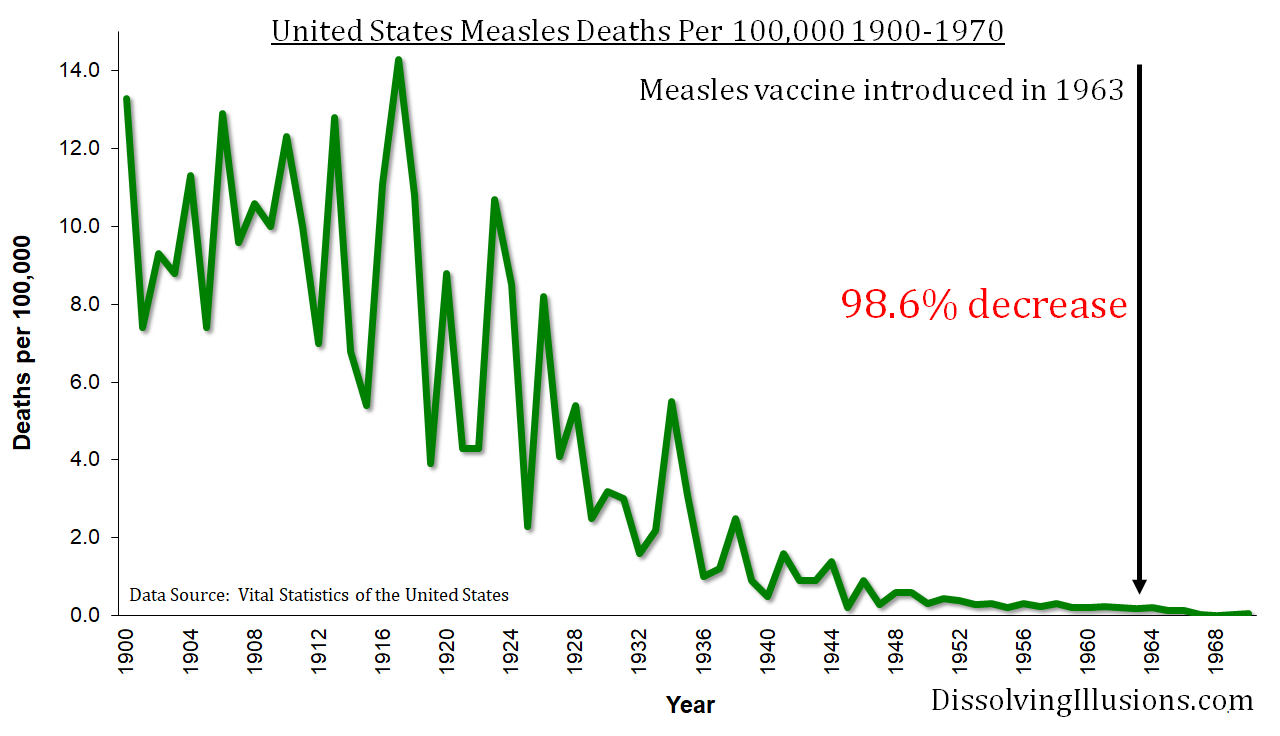
The first measles vaccine in the United States was introduced in 1963. By that point, the death rate from measles had already declined from its peak by 98.7%. This single data point knocks down one of the key cornerstones of the vaccine story.
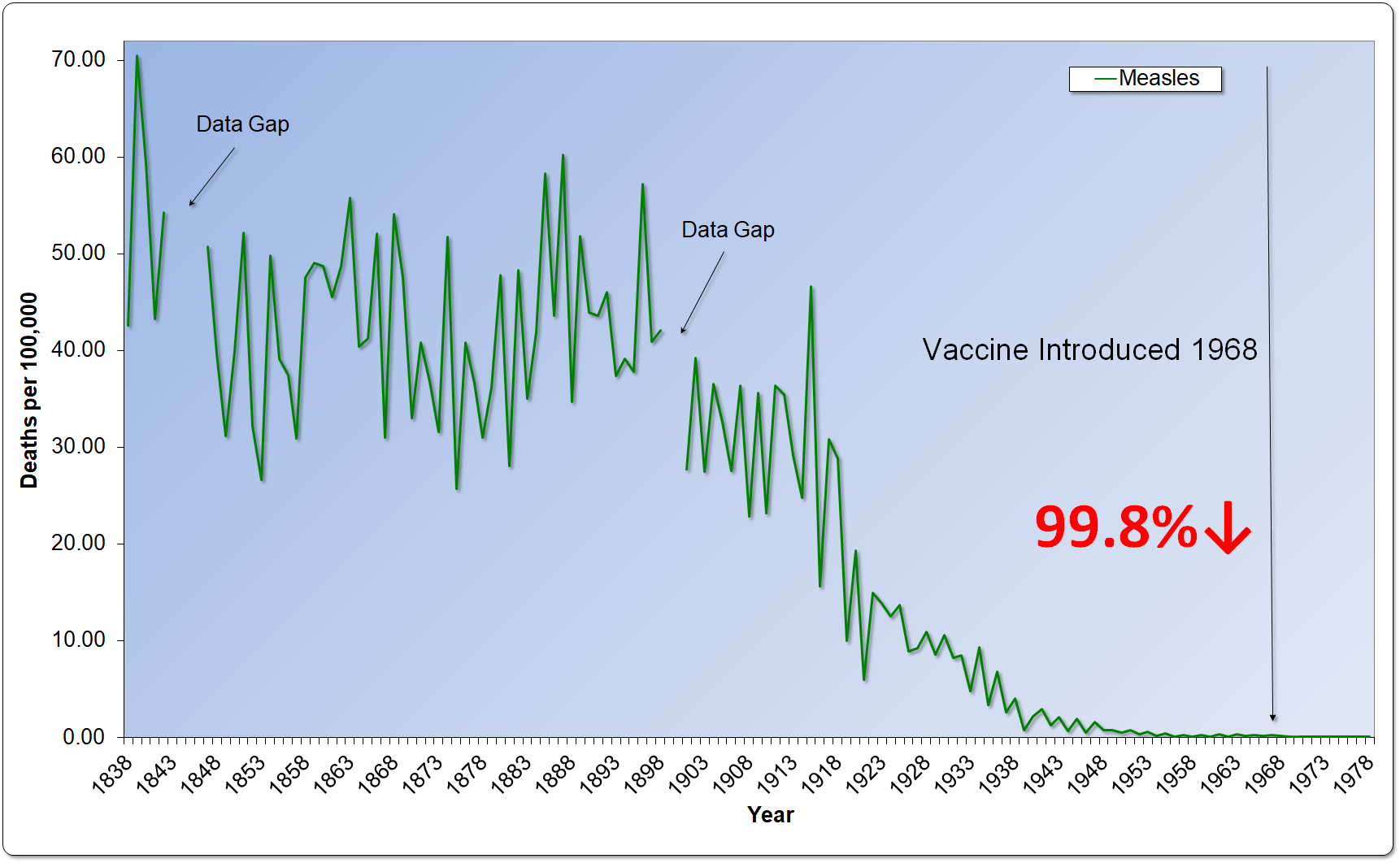
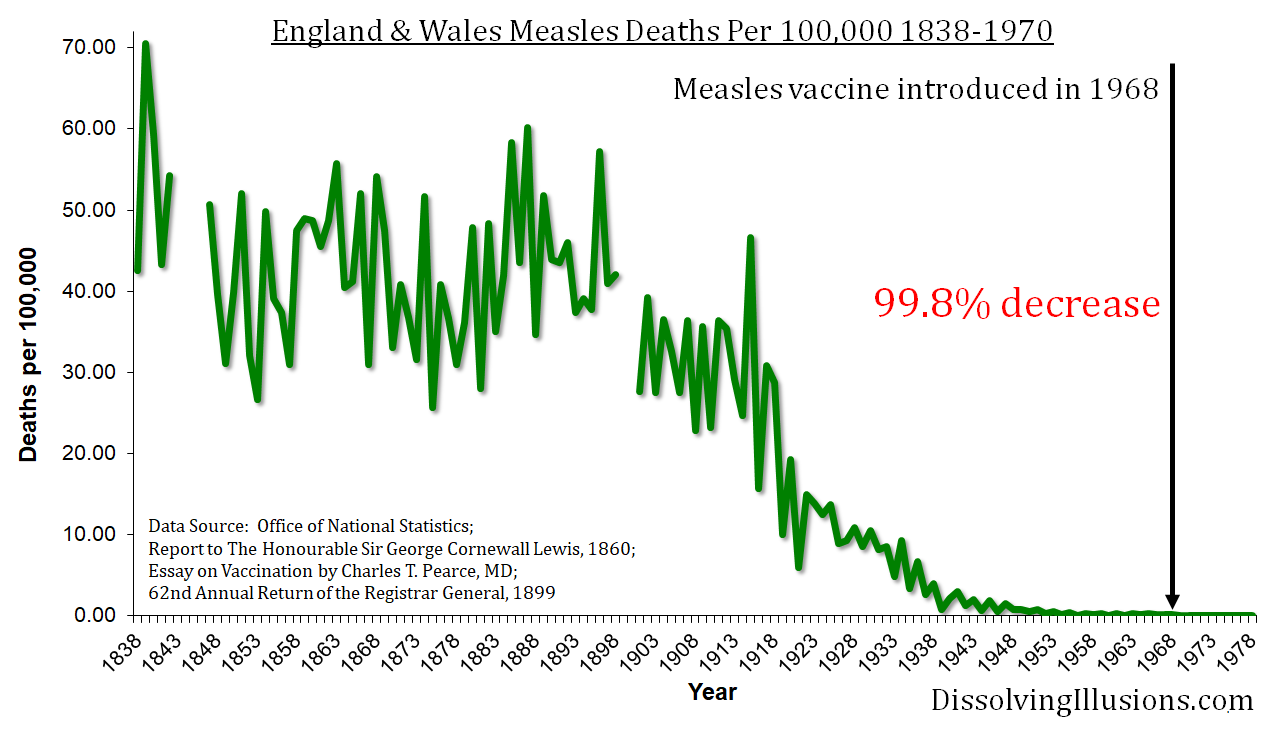
The same phenomenon is observable in England. The English started recording mortality statistics in 1838, and measles deaths plummeted beginning in the late 1800s, reaching nearly zero by the 1950s. Yet it wasn’t until 1968 that England began to vaccinate for measles—five years later than in the United States. By that point, the death rate had declined from its peak by a massive 99.8%—even exceeding the 98.7% decline in the US. In other words, the measles vaccine had little impact on the already greatly reduced death rate.
Importantly, the same steep drop-off in disease mortality occurred before many other vaccines were introduced.
So, then, what was the reason for this reduction in measles mortality if it wasn’t vaccination? As many reports make clear, “The true reason for the massive decline in measles deaths was the improved health of the people. Not any medical intervention, as often is assumed.”
Another persistent distortion arose concerning “pockets in the world where measles are rampant,” with Romania used as a case study. The Roma gypsy example is often cited to induce fear into the population that such outbreaks may hit their communities.
But this claim neglects to explain the context of measles cases among certain Roma people in Europe. It is well-documented that Roma people in Europe experience some of the worst health conditions in the industrialized world. They live in deep poverty, have poor nutritional options, and exist in overcrowded conditions. All these factors lead to severe deficiencies of vitamins A, C, and E as well as other deficiencies associated with malnutrition. Vitamin A deficiency in particular is known to be associated with severe cases of measles in children.
Alongside all kinds of misconceptions are further unanswered questions that parents might want addressed by school administrators and public health officials:
- Why are public health officials, who have specific directives and represent vested interests, allowed to mandate decisions about vaccinations to schools and parents?
- Why must unvaccinated students be quarantined?
- Why would a child who is already vaccinated not be able to have physical contact with an unvaccinated child if the vaccine confers immunity from a disease?
- What if some parents are unconcerned about their child contracting measles? Perhaps they believe if the child contracts measles, they will develop natural immunity and will be spared from ever being infected with measles again.
- Why are schools allowed to make these health decisions for students in lieu of the parents making these kinds of decisions for their own children?
Action Steps: What You Can Do
As evidenced in the Idaho SWHD meeting, certain “truths” die hard, particularly those that have been embedded in our human consciousness by “trusted” institutions over many generations. False assumptions are more quickly put to rest when informed citizens get involved in decision-making processes and take action to educate others.
The June 25, 2024, Idaho SWDH meeting sends a message to citizens that in the current climate the doors are wide open for citizens to take active roles in “all matters relating to public health policy.”
If you live in Idaho, please contact the health board for the district in which you live. Links to all Idaho districts and board members can be found here:
- Contact Idaho board members (District 1, District 2, District 3, District 4, District 5, District 6, District 7) to express your opinions about the proposed measles response plan;
- Contact individual board members directly to discuss and educate them on the facts about measles “outbreaks,” the reactivity of the MMR vaccines, the timeline of vaccinations and measles mortality rates (here and here), the reasons for the oft-cited measles within the Romanian gypsy community, and multiple other historical examples of misinformation;
- Go to health board meetings with sourced information and charts that show conclusively that the nearly complete eradication of the measles occurred long before vaccination began;
- Hold public teach-ins on the issue in your local community;
- Contact the local sheriff’s and prosecuting attorney’s offices, educate them using the above information, and ask them for their public statement on this issue.
Educate yourself, educate others, and don’t allow yourself to be a victim of scare tactics by health bureaucrats. Get involved!













{kind=link}
{kind=link}
{kind=link}
{kind=link}